

This article, originally published on our blog at www.dkchiroblog.com, provides a more in-depth look at understanding back pain. While it’s not an easy read, this article gives support to those who wonder why back pain exists and if chiropractic care has some foundation for treating the cause or source of back pain.
Architectural Mechanical History
For thousands of years, people have built incredible structures around the world — the pyramids of Egypt, temples across Asia and India, and the breathtaking cathedrals of Europe. These buildings were created without electricity, power tools, or modern technology, yet they still stand today. They are a lasting reminder of the brilliance of ancient architecture.
When we look at these wonders, one question naturally comes to mind: how was any of this possible? Laborers didn’t have modern equipment, clean water systems, or proper medical care. Yet, the results of their efforts remain visible centuries later.
One reason is simple: these buildings were constructed on solid foundations.
But when that foundation is compromised, even the greatest structures begin to fail. The Leaning Tower of Pisa in Italy is a perfect example. Construction began in 1173, and by the time it was finished nearly 200 years later, the tower had developed a four-degree tilt. Over the centuries, the lean worsened, creating a very real risk of collapse.
Fast forward to modern times and we see a similar problem with the Millennium Tower in San Francisco. This 58-story skyscraper, opened in 2009, began tilting within just a few years. By 2016, residents were informed that the building was sinking, and by 2022 the lean had reached nearly 28 inches. Engineers have been working ever since to stabilize it, but the solutions are neither simple nor guaranteed.
The message is clear: without a strong foundation, even the most impressive structures are vulnerable.
So, what does this have to do with the human body and back pain?
Like buildings, our bodies also rely on strong foundations. But unlike buildings, our posture is not purely mechanical. Humans don’t simply topple over when they lean or shift. Instead, we adapt, using muscles and balance to stay upright. This unique system allows us to walk, run, bend, and twist without falling.
However, those same adaptations create stress when the body is misaligned. Poor posture, repetitive movements, and uneven mechanics force the spine to carry loads in ways it wasn’t designed to. Over time, that stress accumulates, leading to chronic back pain, disc problems, and sciatica.
In architecture, cracks appear in walls when a foundation fails. In the human body, pain is often the first warning sign. Understanding back pain starts with recognizing that the spine — like a building — depends on a stable foundation for long-term strength.
Levers
Upright human posture is a first-class lever mechanical system. When humans lean (tilt), in any direction, muscles contract in a manner to counter-balance the lean, thus keeping the human upright. A review of these biomechanical principles will further support an effort in understanding back pain.

The first-class lever mechanical system has three components:
- Weight – the load that needs to be balanced (for example, your upper body or something you’re lifting).
- Fulcrum – the central pivot point that supports the system. In the human body, this is the intervertebral disc in the spine.
- Effort – the force needed to counterbalance the load, supplied by muscle contraction.
In the first-class lever mechanical system, the fulcrum is between the weight and the effort. The fulcrum is the site of greatest mechanical stress.
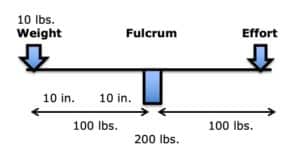
In this model, weight is important. But, more important than weight is the distance the weight is from the fulcrum. This is load. To maintain upright posture, the load must be counterbalanced by effort on the opposite side of the fulcrum. This effort is supplied by muscle contraction. For example:
If you’re holding a 10-pound object 10 inches away from your spine, the effective load on your disc isn’t 10 pounds. Instead, it multiplies to 100 pounds (10 x 10). To keep you upright, your muscles must generate an equal force on the opposite side. That means the total pressure on your spine in this situation is 200 pounds.
In summary, the load experienced at the fulcrum of a first-class lever system is dependent upon three factors:
- The magnitude of the weight
- The distance the weight is away from the fulcrum (lever arm)
- The addition of the counterbalancing muscle effort required to remain balanced
In the low back, the fulcrum of the first-class lever of upright posture is primarily the intervertebral disc. In the low back, the facet joints bear very little weight. In the low back, postural distortions primarily affect the lumbar spine intervertebral discs. Understanding back pain requires further insight into the workings of the spine, including especially the discs.
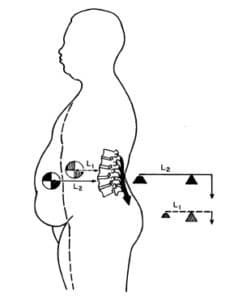
In their 1990 book Clinical Biomechanics of the Spine, Augustus White, MD, and Manohar Panjabi, PhD, state:
“The load on the discs is a combined result of the object weight, the upper body weight, the back-muscle forces, and their respective lever arms to the disc center.”
In her book Move Your DNA: Restore Your Health Through Natural Movement, biomechanist Katy Bowman clearly explains the difference between weight and load, emphasizing that the real problem is the load, which is the weight multiplied by a lever distance from a fulcrum, and of course adding the counter-balancing efforts of muscles. She states:
“The loads created by gravity depend upon our physical position relative to the gravitational force.”
The load created by gravity differs depending on alignment with the “perpendicular force of gravity.”
“Every unique joint configuration, and the way that joint configuration is positioned relative to gravity, and every motion created, and the way that motion was initiated, creates a unique load that in turn creates a very specific pattern of strain in the body.” This is called “load profile.”
“It’s not the weight that breaks you down, it’s the load created by the way you carry it.”
“Loads are often oversimplified to ‘weight’ because it makes them easier to understand, but there is much more going on with your sore knee (or foot, or back, or pelvic floor) than your weight.”
“Weight is not the be-all and end-all of loads. When you want to improve your health, it’s much more important to consider how you carry your weight than to spend hours contemplating the lone data point that is Your Weight.”
The Intervertebral Disc
(the fulcrum)
At the heart of the spine’s mechanics lies the intervertebral disc. These discs act like cushions between the bones of the spine, absorbing shock and helping us bend and twist. But while they are incredibly important, they are also one of the most common sources of chronic back pain.
Research shows that chronic low back pain is often discogenic — meaning it originates in the discs themselves. And while discs are tough, they have a weakness: they are especially vulnerable to rotational stress.
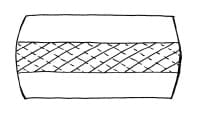
The outer layer of the disc, called the annulus, is made up of fibers arranged in crisscrossing layers. When the spine twists, half of those fibers are pulled tight, while the other half go slack. This means the disc is only operating at half its strength when under rotational stress. Over time, this makes it more likely to tear, wear down, or degenerate.
Crossed Annular Fibers of the Intervertebral Disc
A common cause of chronic rotational stress on the L5-S1 intervertebral disc is postural pelvic unleveling. This was established in 1983 in a study where standing radiographs of the pelvis and lumbar spine were exposed in 288 consecutive patients with chronic low back pain and in 366 asymptomatic controls. Findings showed that 73% of the subjects assessed had meaningful inequality of a lower limb (>5 mm shortness), resulting in pelvic unleveling. The incidence of pelvic unleveling in LBP patients was significantly higher than in asymptomatic controls (more than twice as much).
The counter-rotational stresses on the L5-S1 intervertebral disc:
Axial View From Above
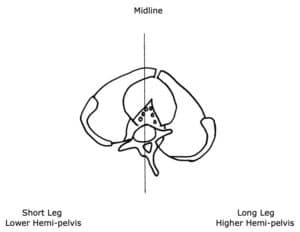
- The L5 spinous process will rotate to the right of midline, towards the side of the long leg and/or higher hemi-pelvis. This causes a counterclockwise rotation of the L5-S1 intervertebral disc.
- The pubic symphysis and pelvis will also rotate to the right of midline, also towards the side of the long leg and/or higher hemi-pelvis. Because the pubic symphysis is in the anterior, this causes a clockwise rotation of the pelvis and sacrum, and a clockwise rotation of the L5-S1 intervertebral disc.
- This results in “significant” counter-rotational stresses, primarily at the L5-S1 intervertebral disc. The consequences of these counter- rotational stresses at the L5 disc are accelerated disc degeneration and degradation, back pain, and sciatica. Such aberrant biomechanics, especially when chronic and even when asymptomatic, predispose the intervertebral disc to injury and pain.
Understanding back pain requires a perspective on the many parts involved. It also requires an understanding of the many connections among those parts, including those areas where things can go wrong.
One of the most famous examples of someone struggling with chronic back pain is U.S. President John F. Kennedy. From his teenage years, Kennedy dealt with poor health and recurring back problems. While serving in the military during World War II, he reinjured his back, and the damage never fully healed.
Throughout his life, Kennedy underwent multiple surgeries, including spinal fusions. Instead of helping, these surgeries often made things worse. He experienced infections, slow healing, and periods of being unable to walk without assistance. Despite access to some of the best surgeons and medical facilities in the world, his back pain remained a constant struggle.
The turning point came when doctors realized his pain wasn’t just the result of injuries or weak muscles — it was mechanical. Kennedy had a leg length difference, which tilted his pelvis and placed uneven stress on his lower spine. By using a heel lift in his shoe, his pelvis was leveled, reducing stress on the discs and giving him more relief than surgery ever had.
Kennedy’s case is a powerful reminder that back pain is often about how the body is aligned, not just about injury or disease. Sometimes, the most effective solutions are the simplest ones, focused on mechanics and posture rather than invasive interventions.
This principle is the foundation of chiropractic care today: fix the imbalance, and the pain often resolves naturally.
The Secretary of the Navy stated:
“For extremely heroic conduct as Commanding Officer of Motor Torpedo Boat 109 following the collision and sinking of that vessel in the Pacific War area on August 1–2, 1943. Unmindful of personal danger, Lieutenant Kennedy unhesitatingly braved the difficulties and hazards of darkness to direct rescue operations, swimming many hours to secure aid and food after he had succeeded in getting his crew ashore. His outstanding courage, endurance and leadership contributed to the saving of several lives and were in keeping with the highest traditions of the United States Naval Service.”
When Kennedy and his crew were eventually rescued on August 8, 1943, Kennedy was non-ambulatory. He was given a cane to help him up. That cane, along with a picture of Kennedy using it, can be seen in the Smithsonian Museum in Washington, D.C.
Despite his back injury, Kennedy only took a month off before returning to command another PT boat. As a consequence of his back injuries, Kennedy was relieved of command on November 18, 1941. He spent months at a military hospital recovering from his back injuries. Because of his low back physical disability, Kennedy was honorably discharged on March 1, 1945.
In 1946, Kennedy was elected to Congress. In 1952, Kennedy was elected to the Senate. During these years, Kennedy’s back problems continued to worsen.
In 1954, Senator Kennedy underwent a spinal fusion operation:
This fusion operation resulted in chronic infection and the surgical wound was not healing. In February 1955, in yet another operation, the fusion hardware was surgically removed. Kennedy remained non-ambulatory through May of 1955. In desperation, Kennedy was referred to an internal medicine cardiologist from Cornell University, Janet Travell, MD.
The physician most responsible for Kennedy’s improvement was Dr. Janet Travell. While many of her peers focused on surgery and medication, Dr. Travell took a different approach. She believed that posture, muscle imbalance, and biomechanics played a much larger role in chronic back pain than most doctors realized.
When she examined Kennedy, she identified his leg length difference and immediately prescribed a heel lift to correct it. She also recommended lifestyle adaptations, like the now-famous rocking chair Kennedy often used, which helped ease pressure on his spine.
Her approach was groundbreaking because it shifted the focus away from endlessly treating symptoms and toward fixing the actual causes of pain. By addressing mechanical stress on the lumbar spine, she helped Kennedy achieve a level of function and relief that surgeries had failed to provide.
Today, her philosophy continues to guide chiropractic care. Chiropractors also emphasize correcting imbalances, restoring posture, and reducing the unnecessary loads placed on the spine. Just like Dr. Travell, they look for the mechanical sources of pain, not just the symptoms, and work to resolve them naturally.
At Dr. Travell’s direction, Senator Kennedy spent his 38th birthday in the hospital. Neurosurgeons T. Glenn Pait and Justin T. Dowdy note:
“In 1955, Kennedy was introduced to Dr. Janet Travell, a Cornell University pharmacologist and internal medicine specialist.”
“Dr. Travell promptly admitted Senator Kennedy to the New York Hospital-Cornell Medical Center to jump-start his rehabilitation program.”
“[Travell] introduced Kennedy to what would, in a few short years, become a symbol of his presidency—the rocking chair.”
“More importantly, it marks the end of his major back surgeries and a shift in focus toward muscular and environmental factors contributing to his back pain.”
“The emphasis regarding treatment of his back would move in a more cautious direction going forward, and notable functional restoration would be seen over the next few months.”
Importantly, Drs. Pait and Dowdy also note:
“In addition to the rocking chair, Travell made other changes, including providing Kennedy with a heel lift— raising the possibility of pelvic obliquity and leg-length discrepancy as a contributing factor in Kennedy’s low back pain.”
In 2003, Dr. Travell’s daughter wrote:
“Senator Kennedy received so much relief of pain from my mother’s medical treatments that he had ‘new hope for a life free from crutches if not from backache’.”
In 2003, James Bagg wrote this, pertaining to Dr. Travell:
“Jack Kennedy saw a great many physicians over the course of his short life, but one of them, according to his brother Bobby, enabled Jack to become President of the United States.”
Kennedy considered Travell to be a medical genius. When Kennedy was elected to the presidency of the United States, he asked Dr. Travell to be his personal White House Physician, becoming the first woman and one of the few civilians (non-military) to hold that post. After President Kennedy’s assassination in 1963, his successor, President Lyndon B. Johnson, asked Dr. Travell to stay on in the White House as his physician. A year and a half later, she resigned to return to private practice and to the position of Associate Clinical Professor of Medicine at George Washington University. She became Emeritus Clinical Professor of Medicine from 1970–1988 and Honorary Clinical Professor of Medicine from 1988 until her death in 1997. Dr. Travell remained professionally active until the end of her life, writing articles, giving lectures, and attending conferences.
In her writings and books, Dr. Travell recognized that a common yet overlooked “perpetuating factor” for chronic discogenic back pain and counterbalancing muscular stress was a structural difference in the length of the lower limbs. It has been documented since 1946 that about 75% of people have legs of unequal lengths, and that about a third of people have leg length differences that contribute to chronic back pain. As a rule, the sacrum is lower on the side of the short leg (see drawing below). The spinal column initially tilts towards the short leg, then compensates back to the midline as a consequence of chronic contraction of the quadratus lumborum muscle.
Posterior to Anterior View From Behind
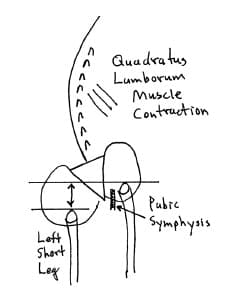
Understanding back pain can also involve a perspective on biomechanics where the parts do not sit or move as they should. In this instance:
- The sacrum is lower on the side of the short leg (left in this drawing).
- The spinal column initially tilts towards the short leg, then compensates back to the midline as a consequence of contraction of the quadratus lumborum
- The lumbar spinous processes (posterior) rotate towards the long leg. The pubic symphysis (anterior) also rotates towards the long leg. The consequent counter-rotational forces abnormally stress the L5 intervertebral disc.
Dr. Travell noted that the solution was a proper heal lift, inserted into the shoe with the goal of leveling the pelvis and removing the counter-rotational stress of the L5 intervertebral disc. This intervention was included in her management of Senator Kennedy.
SUMMARY
Understanding back pain requires more than a look at symptoms — it requires examining the foundation of the spine itself. Just as great buildings collapse without a strong base, the human spine suffers when posture, balance, and alignment are off.
From the biomechanics of levers and intervertebral discs, to the historical lessons of President John F. Kennedy’s struggles, the message is clear: chronic back pain often stems from structural and mechanical causes. Correcting posture, leveling the pelvis, and reducing disc stress are essential for long-term relief.
Modern chiropractic care in Toronto follows this same path. By addressing posture, balancing the pelvis, and protecting the intervertebral discs, chiropractors don’t just manage back pain — they correct the underlying mechanics so patients can move better, feel stronger, and prevent future problems.
If you are living with chronic back pain in Toronto, chiropractic treatment may be the solution. With a focus on restoring balance and protecting the spine, chiropractic care offers a safe, natural, and effective approach to reducing pain and improving quality of life.
*****
Frequently Asked Questions About Back Pain
What causes chronic back pain?
Chronic back pain can be caused by many factors, including poor posture, disc degeneration, sciatica, pelvic imbalance, or even differences in leg length. Over time, these imbalances place uneven stress on the spine, especially the lumbar discs, leading to persistent pain.
Can chiropractors help with lower back pain?
Yes. Chiropractors specialize in diagnosing and treating the mechanical causes of back pain. By correcting posture, restoring spinal alignment, and addressing pelvic tilt or muscular imbalances, chiropractic care can relieve lower back pain and prevent it from returning.
Is back pain always caused by a herniated disc?
No. While disc problems can cause significant pain, many cases of back pain are due to stress on the muscles, ligaments, and joints of the spine. Chiropractic care looks at the whole picture — discs, posture, and biomechanics — to find the true source of pain.
When should I see a chiropractor for back pain?
If your back pain lasts more than a few days, interferes with daily activities, or keeps returning, it’s a good idea to consult a chiropractor. Early treatment helps prevent minor issues from turning into long-term chronic back pain.
Do I need a referral to see a chiropractor in Toronto?
No. Chiropractors in Toronto are primary health care providers, which means you can book an appointment directly without a referral. Many patients seek chiropractic care for back pain as their first line of treatment.
*****
Our office is a member of ChiroTrust and has taken The ChiroTrust Pledge:
.
“To the best of my ability, I agree to provide my patients convenient, affordable, and mainstream Chiropractic care. I will not use unnecessary long-term treatment plans and/or therapies.”
.
Toronto Neck and Back Pain Clinic
1849 Yonge Street #412 Toronto ON M4S1Y2
www.DKChiroBlog.com
.
Open:
Mon 8-10, 12-1, 3-6
Tue 8-10, 12-1
Wed 3-6
Thu 8-10, 12-1, 3-6
.
Walk-Ins Welcome or To Make an Appointment,
Call 416-960-9355
Or visit www.torontoneckandbackpain.com



